
Women with dense breast tissue are more likely to get cancer, a new study has confirmed.
Researchers using automated breast density measurements have found that women with mammographically dense breast tissue have higher recall and biopsy rates and increased odds of screen-detected and interval breast cancer.
Norwegian researchers say their findings, published online by the journal Radiology, support automated measurements as a future standard to ensure objective breast density classification for breast cancer screening.
Previous studies have shown that women with mammographically dense breasts face a higher risk of breast cancer and missed cancers than those with non-dense breasts.
This is partly because the superimposition of dense breast tissue on mammograms leads to a masking effect, causing some cancers to go undetected.
But the majority of those studies relied on subjective density assessments – most commonly, the radiologist’s subjective interpretation using the American College of Radiology’s Breast Imaging Reporting and Data System (BI-RADS).
That approach introduces potential mammogram reader variability into density categorisation, said the study’s principal investigator Ptofessor Solveig Hofvind, of the Cancer Registry of Norway.
For the new study, Prof Hofvind and her colleagues used automated software to help classify mammographic density in 107,949 women aged 50 to 69 from BreastScreen Norway, a national programme that offers women screening every two years.
The researchers looked at a total of 307,015 digital screening examinations that took place from 2007 to 2015.
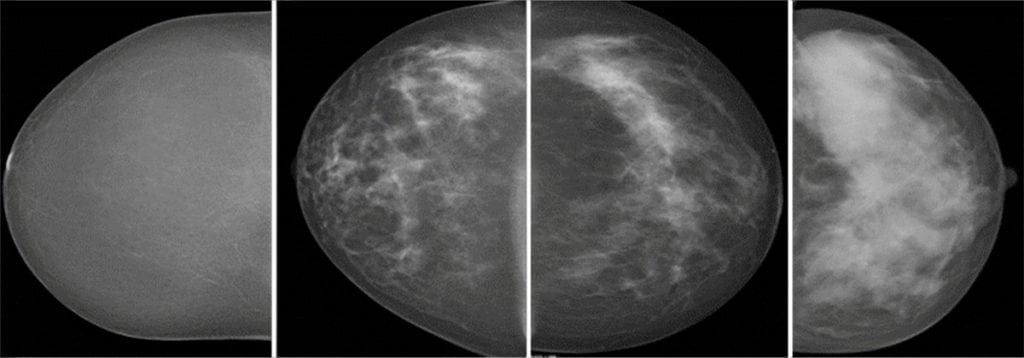
The automated software classified breasts as dense in 28 per cent of the screening examinations.
Rates of screen-detected cancer were 6.7 per 1,000 examinations for women with dense breast tissue and 5.5 for women with non-dense breasts.
Interval breast cancer, or breast cancer detected between screenings was 2.8 per 1,000 in the dense breast tissue group and 1.2 for women with non-dense tissue.
The recall rate, or rate at which women are called back for additional examination based on suspicious mammographic findings, was 3.6 per cent for women with dense breasts, compared with 2.7 per cent in women with non-dense breasts.
The biopsy rate of 1.4 per cent in the dense breasts group was higher than the 1.1 per cent rate for women in the non-dense category.
Prof Hofvind said: “The odds of screen-detected and interval breast cancer were substantially higher for women with mammographically dense versus fatty breasts in BreastScreen Norway.
“We also found substantially higher rates of recalls and biopsies among women with mammographically dense breast tissue.”
Mammographic sensitivity for detecting breast cancer was only 71 per cent for women with dense breasts, compared to 82 per cent for women with non-dense breasts.
Cancers detected at screening were more advanced among women in the dense breast tissue group.
Average tumor diameter for screen-detected cancers was 16.6 millimetres in the dense breasts group, compared to 15.1mms for the non-dense group.
Lymph-node-positive disease was found in 24 per cent of women with dense breasts, compared with 18 per cent for women with non-dense breasts.
Prof Hofvind noted that more than half of states in the U.S. have enacted breast density legislation, with some states requiring that women be informed about their breast density or that additional imaging could be beneficial.
But supplemental screening for women with dense breasts currently is not recommended by any of the major health care societies or organisations.
Prof Hofvind added: “We need well-planned and high-quality studies that can give evidence about the cost-effectiveness of more frequent screening, other screening tools such as tomosynthesis and/or the use of additional screening tools like MRI and ultrasound for women with dense breasts.
“Further, we need studies on automated measurement tools for mammographic density to ensure their validity.”
Dr Liane Philpotts, of Yale School of Medicine in the US, said of the findings: “This study is important for two main reasons: firstly, the validation that automated means of density classification can correctly identify a percentage of women with dense tissue.
“And, secondly, women with dense tissue have poorer performance of screening mammography. It lends support to the density notification movement along with redoubling efforts towards optimising supplemental screening methods.”
She added that automated volumetric determination could better standardise density measurements and provide greater confidence that women with dense breast tissue could consistently be identified.
Dr Philpotts added: “Breast density is here to stay, and it is in everyone’s best interest to embrace understanding and optimisation of breast imaging practice to best address the needs of women with dense tissue.”
https://www.thelondoneconomic.com/lifestyle/health/cancer-could-be-stopped-in-its-tracks-within-the-next-few-years/22/06/